If you have the opportunity to go to the AcademyHealth Dissemination and Implementation annual conference, I highly recommend attending a coffee chat or two. It took me awhile to discover the hidden gem. (They are not really “hidden.” They are just at 7 am. When I attend a conference, I prefer a 9 am start time to ease into the day—and I’m not even coming from the Pacific time zone like so many of our colleagues! However, coffee chats are worth rising early.) They focus on one area in D&I science and are led by experts in that topic area. The general format is that the leaders of the coffee chat set the stage for where the field is at in that particular topic area and then they open it up for everyone who attends to ask questions and share their experiences around the topic.
This past annual meeting in December, I attended one on mechanisms led by Cara Lewis, Byron Powell, and Brian Mittman. I have struggled with the turn towards mechanisms in implementation science. I know I need to do a deep dive into the area but have not yet had the opportunity to take that dive. The coffee chat was a great way to enter the conversation.
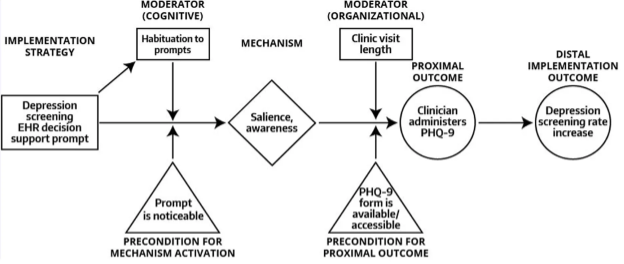
Before attending, my only formal engagement with mechanisms was Cara Lewis and colleagues 2018 perspective piece, From Classification to Causality: Advancing Understanding of Mechanisms of Change in Implementation Science. In the article, they define a mechanism as “a process or event through which an implementation strategy operates to affect desired implementation outcomes” or “all pathways through which a strategy’s effects take place.” They also layout four steps for mapping causal pathways from the implementation strategy to the implementation outcome, which includes particular focus on moderators and the mechanism through which the implementation strategy influences the implementation outcome (See Figure from article).
During the coffee chat, I listened to learn all the different ways people talked about testing mechanisms in implementation science studies. Then Lisa Hirschhorn shared about an implementation study they were conducting in several countries in Africa. I’m sorry to say I don’t remember the details of the study, but I do remember her sharing how they had to change the implementation strategies because in one country the hospitals had a strong hierarchy where physicians were positioned at the top, whereas in another country the nurses and physicians worked much more collaboratively. She talked about the challenges of breaking these scenarios into specific mechanisms and subsequent changes in implementation strategies. I remember thinking, “That is culture.”
I then raised my hand and said, “I’m a medical anthropologist. I have tried very hard to understand form and function, mediators and moderators and mechanisms, but I don’t think mechanistically.”
Since that time, I’ve been trying to disentangle what I meant when I said, “I don’t think mechanistically.” Do I mean I don’t think causally? Do I mean I don’t think about behavior change as discreet mechanisms like self-efficacy or salience (from the example in the Figure)?
In some ways, the simple answer is yes. My brain sees interconnected complexities that require description rather than testing. At the same time, I have used workflows in studies. If I look back at those, could I see mechanisms, mediators, and moderators?
I don’t know if you remember my reflection in December, but I said I’m feeling less like I have a home in implementation science—and at the same time I’m committed to a deeply interdisciplinary, multi-method field.
What I need help with is how I learn to think differently—even temporarily—so I can be a more effective partner in the mechanism conversation, while at the same time maintaining where I see my strengths as an ethnographer.
I’m in the midst of an incredible opportunity to engage in this interdisciplinary thinking surrounding mechanisms. I look forward to sharing more in the future—and when the publication is out for public viewing!